UnitedHealthcare, the country’s largest healthcare insurance provider, has transitioned their guidelines for determining level of care for hospitals from MCG Care Guidelines (MCG) to InterQual® clinical criteria. This change took place on May 1st, 2021. The shift included nearly all their commercial, Medicare Advantage and Medicaid benefit plans. This was a big change for hospitals with a large population of United Healthcare patients.
What are the differences between InterQual® and MCG criteria?
There are differences in how they are laid out and how they are viewed. Further, as summarized by a revenue recovery organization, “the criteria set out in MCG is less precise, leaving room for interpretation. On the other hand, InterQual ® is very specific and detailed in setting criteria for both severity of illness (citing precise vital sign abnormalities, lab values, test results, etc.) and intensity of service (specific treatments/treatment plan that must be done) to meet inpatient level of care.”(InterQual® vs. Milliman Care Guidelines. April 29, 2021. https://www.myadvicare.com/post/interqual-vs-milliman-care-guidelines).
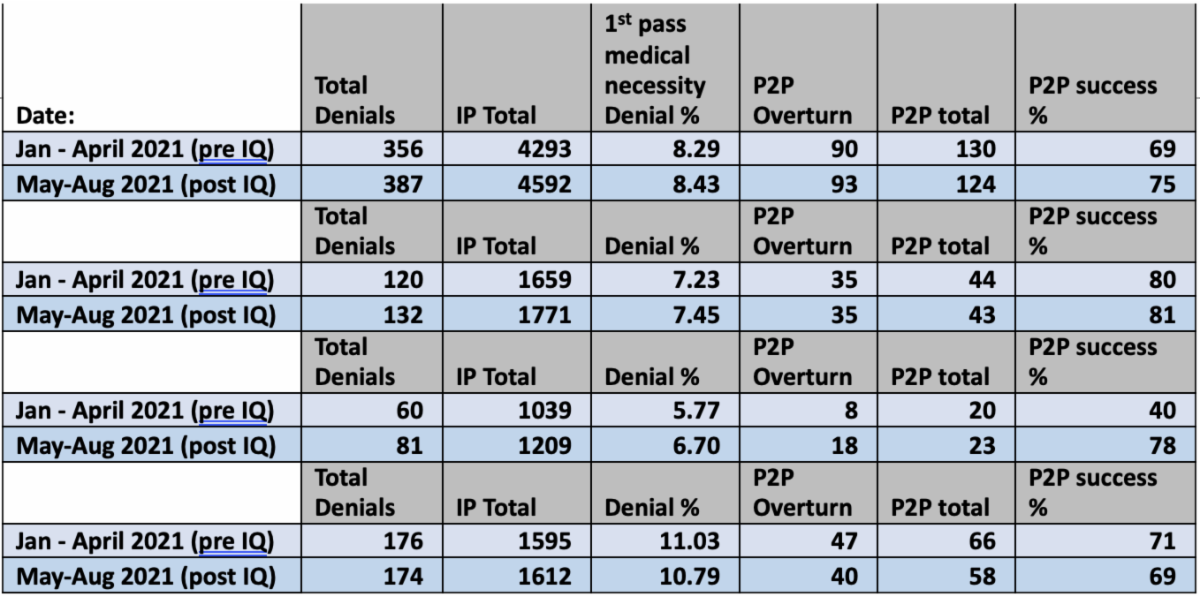
At University Hospitals in Northeast Ohio, we sought to answer how United HealthCare’s change to InterQual® has impacted our institution. We looked at our data 4 months pre-, and 4 months post-adoption of InterQual® by United Healthcare, in terms of overall denial rates, total peer-to-peers performed, and rate of peer-to-peer success. In addition to examining UHC as an organization, we broke it up by each individual UHC participant, namely commercial, Medicaid, and Medicare Advantage, as presented sequentially in this table.
UH data: 4 months pre and post UHC adoption of InterQual®: