The anatomical components of MS-DRG include:
1) Principal Diagnosis
Uniform Hospital Discharge Data Set (UHDDS) defines Principal Diagnosis (PDx) as the condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care. This may not be identical to the admitting diagnosis (e.g., admitted for abdominal pain but, after study, PDx is determined to be acute cholecystitis).
For the most part, the principal diagnosis drives the DRG assignment. On certain occasions where a surgical procedure is performed, or pregnancy status is reported, the principal diagnosis might not be the sole driver for the DRG assignment. Secondary diagnoses impact the DRG assignment as well by adding a CC and/or MCC when clinically valid, supported, and consistently documented.
2) Secondary Diagnoses
UHDDS defines secondary diagnoses as all conditions that coexist at the time of admission, that develop subsequently, or that affect treatment received and / or length of stay.
3) Comorbid Conditions or Complications
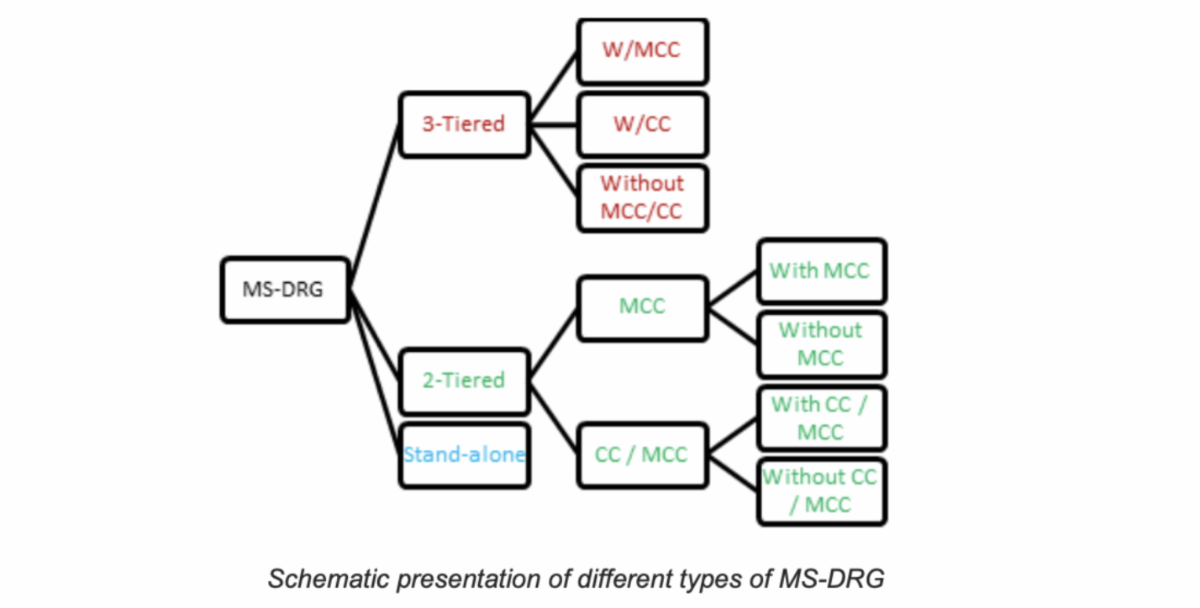
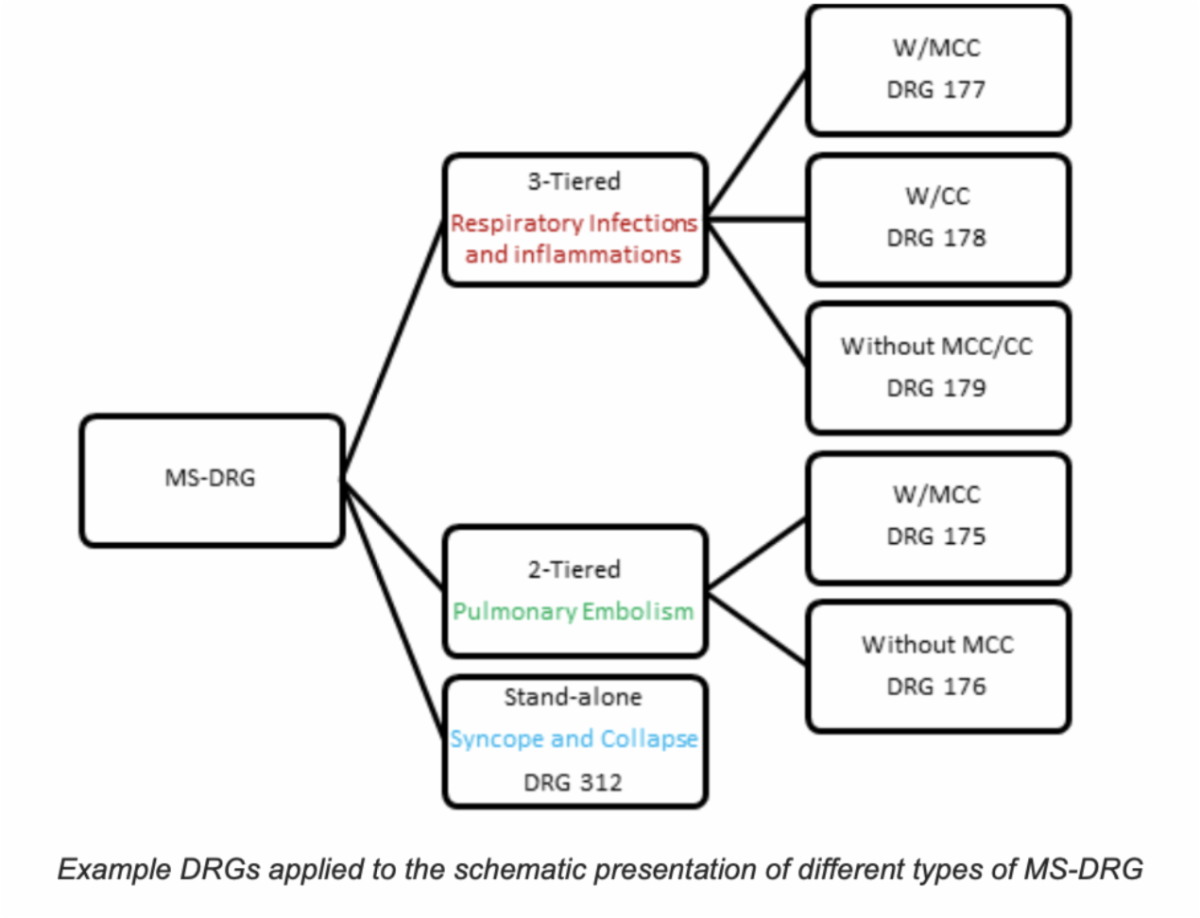
Some secondary diagnoses are designated as risk-adjusting comorbid conditions or complications (CCs). Others considered even more serious are referred to as major comorbid conditions or complications (MCCs). CCs and MCCs indicate a higher severity of illness, risk of mortality, and intensity of resource utilization. These CCs and MCCs define many of the tiered MS-DRG sets. It only takes one CC or MCC to establish the tier. Although it is optimal to capture all the CCs/MCCs present, having more than one in a given tier does not have any greater impact.
Examples of CCs include chronic respiratory failure (hypoxemic, hypercapnic, or combined), chronic congestive heart failure (systolic, diastolic, or combined), acute kidney injury, hyponatremia, and moderate protein-calorie malnutrition. Examples of MCCs include acute or acute on chronic respiratory failure (hypoxemic, hypercapnic, or combined), acute or acute on chronic congestive heart failure (systolic, diastolic, or combined), pneumonia, and severe protein-calorie malnutrition.
4) Relative Weight (RW)
RW is a measure which reflects the relative resource consumption (cost) associated with treatment of that condition as compared to the resource consumption of the average Medicare patient (by convention, defined as 1.0000). Each DRG is assigned a specific RW. The Medicare Payment Advisory Committee (MedPAC) reviews hospital claims data annually as part of IPPS annual updates resulting in changes to RW each year. In MS-DRG sets, the relative weight increases with the tier; e.g., RW of DRG with MCC > RW of DRG with CC > RW of DRG without CC or MCC.
5) Case Mix Index (CMI)
CMI is a numeric measure which represents the average DRG RW for that hospital. It is calculated by summing the DRG weights for all Medicare discharges and dividing by the number of discharges. It is used to find and adjust the average care cost per patient at a hospital based on the patient population demographics. For example, if a hospital’s average cost per patient is $2,000 and its annual CMI is 0.90, then the adjusted cost per patient would be $2,222.22. In general, increased capture of MCCs equates to higher CMI. Higher surgical DRGs results in higher CMI as well. To put it in simple words, higher CMI means you are treating sicker, more complex, and more resource-intensive patients.
6) Hospital Base Rate
Hospital Base Payment Rate (Blended Rate) is a monetary number assigned to an individual hospital that allows for adjustment according to individual characteristics of that hospital. It is recalculated annually to reflect differences in operating expenses as well as capital expenses. Factors that impact the hospital blended rate include proportion of indigent population, capital costs, wage index, urban vs rural designation, teaching vs non-teaching designation, and cost of living adjustments. The Hospital Base Rate multiplied by the RW of the MS-DRG determines the payment for a given patient encounter.
7) Length of Stay (LOS)
Arithmetic Mean Length of Stay (ALOS) reflects the average LOS for CMS patients who fall into a given MS-DRG. Geometric Mean Length of Stay (GMLOS) reflects the average LOS for CMS patients who fall into a given MS-DRG with patients with abnormally short or long LOS (called outliers) being removed from the calculation. In tiered DRG sets, the higher the tier, the longer the allotted LOS.
The basic equation which explains the MS-DRG payment is shown below. While we (physicians and physician advisor community) have no direct control over what the updated hospital base rate would be every year, we have control in documenting all clinically relevant and pertinent diagnoses which can risk adjust the MS-DRG (if designated as MCC or CC) leading to a higher RW which will ultimately lead to higher reimbursement.